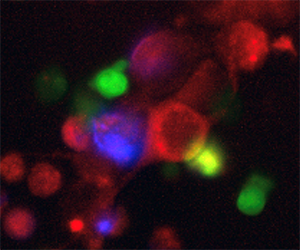
T cells (green) killing cancer cells (red) in a petri dish. Once the cancer cells die, they turn blue.
Know Thy Self

Immunotherapy and the Future of Cancer Treatment
The trouble with cancer is that it’s you. From an immunological standpoint, it’s not a foreign body, but rather a bit of self that has grown wildly, dangerously out of order. A tumor has everything it needs: its own blood vessels, nutrients, and other growth-aiding compounds. All it has to do is “ask” by using the same molecular signals the body uses to identify self and not-self.
By co-opting the immune response, cancers have typically been able to grow unseen and unchecked, but Jefferson is changing this through a multipronged immunotherapeutic effort. Among the many ongoing initiatives are two projects aiming to reverse the co-opted immune response in glioblastoma multiforme (GBM), a particularly dangerous brain tumor, and colorectal cancers. GBM kills about 20,000 people a year in the United States, while colorectal cancers are the second-leading cause of cancer-related death in the country.
“Our brain cells or our skin cells, and the like, they’re all genetically identical to each other,” says Adam Snook, PhD ’08, an immunologist and assistant professor of Pharmacology and Experimental Therapeutics. “But we have these big populations of immune cells that are genetically different from each other and can actually rearrange their DNA to respond to what they’re ‘seeing.’” So great is the variety that researchers speculate that there may be more than a thousand trillion types of immune cells, each geared to respond to a different pathogen.
With such a complement of protectors, it’s not unreasonable to think that the body’s best advocate may be itself. This general orientation informs the technique of immunotherapy, which is—very roughly—twofold: reminding and finding.
The body has forgotten that cancer is not to its benefit, tricked in various ways into ignoring the traitorous cells. As bad as this is, it is nonetheless stable in the sense that it is self-sustaining, and so any treatment must change this condition. Immunotherapies, especially vaccination, do this by stimulating disharmony in this pathological equilibrium, alarming the body’s defenses and then directing this immune attention to the cancerous cells.
How they do this is unique to the type of cancer, and to each researcher’s creativity.
Rabies to Riches
For a surgeon, GBM presents a vexing challenge because of how aggressive the tumors can be. Coming in several variants, the prognosis is anywhere from five to seven years or a few months—maybe disappearing for months and years after a successful surgery and chemo, only to later return.
David Andrews, MD, the Anthony Alfred Chiurco Professor of Neurological Surgery and director of Stereotactic Radiosurgery, was tired of seeing the same story unfold. As he tells it, his work on the vaccine “began at the turn of the century,” not long after the idea of immune intervention went from theoretically to technically feasible. He and his collaborators had the idea to implant small GBM cell-filled containers into mice in an attempt to stimulate an anti-cancer immune response. The containers themselves contained tiny holes, 100 nanometers in diameter—small enough that cells cannot enter or leave, but big enough to allow the immune system to “take a look” at the tumor cells in the hopes that the body may recognize the tumor in its midst.
Andrews and his team noticed some minute effects from this procedure, enough to take things further. They reached out to D. Craig Hooper, PhD, professor of Cancer Biology and member of the Sidney Kimmel Cancer Center, an immunologist who is an expert on neuroimmunology, the blood-brain barrier, and central nervous system diseases like rabies and multiple sclerosis. “I looked at their results and what they had done and decided they were a little crazy,” recalls Hooper. “But there was something there in theory, which made it interesting, so I got involved.”
Working with a mouse brain tumor model as well as blood and tumor samples from Andrews’ patients, Hooper set about figuring out what made GBM tick, teasing out the complex relationship between host and disease. “In cancer, we understand that the immune system is often sick as well, so either the immune system doesn’t recognize cancerous cells as such or that an appropriate immune response is suppressed,” Hooper says. With GBM, the latter was very much the case due to the activity of a type of immune response that is primarily directed at repairing tissue and inhibits therapeutic tumor immunity.
This is what is called a “type 2” immune response, distinct from the more well-known “type 1” reaction wherein white blood cells attack and destroy bodily intruders. In a type 2 response, growth-promoting cells, molecules, and other instruments of repair flock to the site of damage in order to restore order. Among these are M2 macrophages—one of the immune system’s workhorses—set to play a protective role instead of their commonly assigned hunter-killer theme.
When this happens in a cancerous area, like the site of a GBM tumor, the disease begins to grow out of control in spite of the presence of any therapeutic type 1 immune mechanisms. However, Hooper discovered a route of attack—like the tumor cells themselves, the M2 macrophages had a receptor on their surfaces for a molecule called insulin-like growth factor 1 (IGF-1). By using antisense, a complementary “key” that binds to mRNA encoding the IGF-1 receptor, the “help” properties of the M2 macrophages could be turned off, allowing the “attack” type 1 mode of immunity to act.
The team’s treatment protocol closely mirrors standard-of-care approaches, beginning with surgical resection of the GBM tumor. The procedure opens the patient’s blood-brain barrier for a few weeks, giving the peripheral immune system access to the tumor environment and allowing any acquired immunity to flow in. Within 24 hours, 20 micro-chambers—filled with the patient’s tumor cells and antisense molecules—are implanted into the abdomen, acting as stimulus to promote therapeutic anti-tumor immunity.
Says Hooper, “We’re pioneering something that’s very much building a vaccine at bedside.” This combination of antisense-treated tumor cells and free antisense achieves two goals: to present the body with the GBM antigen, so the immune system can ”see” it in the right context, and to switch the body’s immune response from type 2 to type 1.
“The biologics are the patient’s own cancer cells, but the active drug is really the antigens produced by those cells,” says Andrews. “They’re going to be different in each individual, so this is really a highly personalized vaccine.” And the vaccine is doing well in trials, showing reductions in tumor size and increasingly better prognoses for patients. Now the work is to continue testing to find the best possible dosage, timing, patient profile, and numerous other factors.
“All the work I’ve done in mice, MS, and rabies built a lab that was entirely suited to look at brain cancer,” muses Hooper. “Such is the tortuous path of a scientist’s career.”
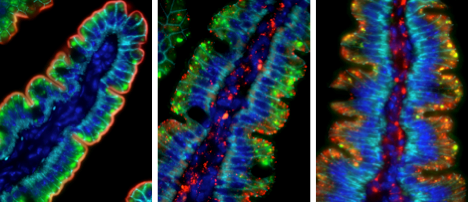 A stain of GCC (green) in the intestinal lining
A stain of GCC (green) in the intestinal lining
Inside Out
“I’m the senior guy on this project,” says Scott Waldman, MD, PhD ’80, chair of the Department of Pharmacology and Experimental Therapeutics. “But in many ways I’m Adam’s collaborator. I’m the GCC guy, but immunology is his wheelhouse.”
GCC, or guanylyl cyclase C, is a receptor that sits on the cells of the intestines’ inner lining (the lumen) that Waldman has spent his career studying. In 1993, he discovered that this molecule would make a good target for diagnosis and therapy due to its highly specific placement. Some years later, Snook, an immunology PhD student at the time, came along wanting to study potential immunotherapeutic approaches to cancer—the molecule had found its vehicle to the clinic.
“It’s fascinating because cancer is technically self,” Snook says. “Our bodies eliminate immune cells that react against self through a process called tolerance. Our challenge is to figure out how to overcome that, to induce an immune response to cancer, but not so much that we create autoimmunity.” With Waldman as mentor, co-investigator, and cheerleader, Snook set out to understand how to pull off this balancing act in order to create a vaccine that will protect colorectal cancer patients from metastases.
One asset in this work is the GCC molecule, which is specific to colon cells, while another came from the world of HIV research. As it turns out, immunity in the mucosal membranes (in the intestines, stomach, and similar tissues) are separate from the rest of the body. Snook and Waldman learned about the difference from other scientists’ work developing HIV vaccines. While researchers had some success inoculating animals via an injection in the muscle, this had no impact on the mucosal membranes, the primary site of exposure in many HIV patients.
“It’s a really amazing system,” Waldman says. “We took advantage of this anatomical and immunological compartmentalization as we were developing our vaccine.” This separation prevents autoimmunity and allows them to target GCC metastases outside the mucosal membrane, essentially teaching the body to attack intestinal cells whenever they’re found outside of the gut.
Originally, they accomplished this by incorporating the GCC molecule into adenovirus type 5, a common, safe, well-understood virus. Once injected, the body rightly recognizes this as an invader and moves to investigate. Similar to the GBM vaccine, when the immune system “looks” at the virus, it sees the GCC compound, making it a candidate for an aggressive immune response if colorectal metastases are found elsewhere in the body.
However, it turned out that adenovirus type 5 is so common that 50 percent of patients already had antibodies for the virus and were too efficient at clearing it before acquiring immunity to GCC. To solve this, Snook and his team replaced the fiber molecule on the viral surface with that from adenovirus type 35, extremely rare in humans, increasing its effectiveness and offering immunity to 90 percent of patients.
Now the plan is to start a large, multiyear trial of the vaccine in colorectal cancers, with the aim of treating about 80 patients to prevent metastases from forming or to help fight recurrent disease. “From the very beginning, I had a lot of support, but also a ton of autonomy. Scott literally told me ‘Here’s a molecule. Cure cancer,’” says Snook. “We’re on the verge of a major milestone together and it has been really exciting to be at this point after nearly 20 years.”

The implants that Andrews and Hooper use to stimulate immunity in GBM patients.