History
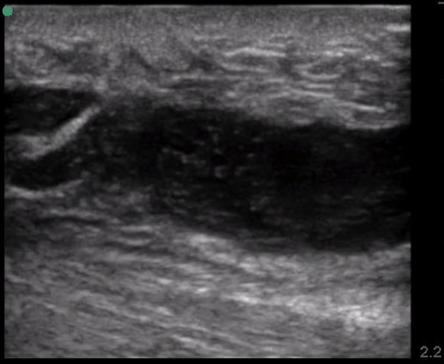
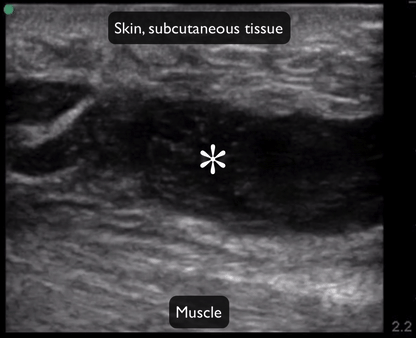
Michael Cooper is a 27-year-old male who presents to the Emergency Department for a “skin infection.” He has been using fentanyl for the last 2 years. He is new to town. He’s had problems like this before, and attributes the arm swelling (and pain) to injecting. His review of systems is otherwise negative. He had asthma as a child but no other active medical problems; his surgical history is significant for a broken left leg from a motorcycle accident approximately 2 ½ years ago. He takes no prescribed medications and has no allergies. He does smoke daily, no alcohol.
You are on your 1st day of your ED clerkship.