CT Angiography (CTA) is a relative new, non-invasive procedure capable of producing high-resolution images of the vascular system using the latest CT imaging technology. The recent development of multi-slice CT scanners capable of rapidly acquiring very thin (fractions of a millimeter) images, and the computer algorithms necessary to assemble large numbers of spiral scans (typically hundreds) into three dimensional images were the key developments that led to the remarkable capabilities of this technique.
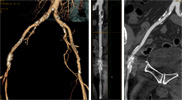
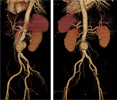
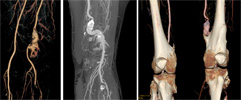
Advantages of CTA compared to standard catheter based angiography include the ability to look at vessels from an unlimited number of angles, and from both inside and outside the vessel wall. Using a variety of imagine techniques such as multiplanar reconstructions, volume rendered (VR) images, and maximum intensity projections (MIP), vessels walls, not just the vessel lumen, can be evaluated. The morphology of atherosclerotic plaque can clearly be visualized, which in come cases may be a more important factor in determining clinical outcome than simply the degree of luminal narrowing.
Since it is less invasive than catheter based angiography, the pre and post procedure requirements associated with conscious sedation are eliminated, the anticoagulation status of the patient is no longer important, there is no post procedure recovery time, and the risks associated with the procedure are greatly reduced.
Visualization of extravascular structures sometimes adds key information about the cause or significance of a vascular problem. Visualization of the soft tissues and skeletal structures provided by CT imaging can be a valuable adjunct to evaluating arterial or venous lesions in some cases.
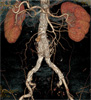
The primary indication for CTA is for the initial evaluation of any patient with suspected vascular disease. Once the vascular anatomy and the site and severity of vascular lesions are demonstrated, the optimal treatment strategy (medical, interventional or surgical) can be determined. Specific indications most commonly include evaluation of patients with symptoms of peripheral vascular disease, but other indications include evaluation of various forms of arteritis, mesenteric or renal ischemia, vascular malformations, or collagen vascular diseases. Preoperative evaluation of aneurysms, and postoperative follow-up of surgical or interventional vascular procedures, such as evaluation of endograft leaks, are also important indications. There are many other less common indications, and new indications are continually being described.
Contraindications include previous severe reactions to radiographic contrast agents, and uncooperative or pregnant patients. The usual precautions for the use of intravenous contrast agents also apply. Vessels adjacent to metal prostheses, such as joint replacements, are not well visualized because of CT artifacts.
The Department of Radiology at Jefferson has some of the most advanced CT scanners and 3D workstations in the country. Jefferson Radiology has a long history of being leaders in vascular imaging and interventional research. Faculty with nationally recognized subspecialty expertise in imaging of vascular disease, and vascular interventions are available for consultations.
For more information, or to schedule a outpatient CTA procedure, call 215-503-4900.