Capillary Malformation (LM)
CMs generally present after birth. CMs are flat, sharply demarcated, red-pink staining of the skin, sometimes referred to as a "port-wine stain". CM’s most commonly involving the head and neck. Most are harmless birthmarks but they can signal an underlying abnormality if they involve the upper eyelid, forehead or overly the spinal column. They are often present as part of combined vascular malformations associated with limb overgrowth. CMs are treated with pulsed-dye laser and are generally not treated by Interventional Radiology techniques.
Combined Vascular Malformations
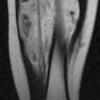
Combined malformations affect the extremities and trunk and are associated with limb overgrowth in both girth and in length. Combined malformations involve more than one tissue/channel type. They can be accompanied by overgrowth of soft tissue and bone in the affected region/extremity. They sometimes affect more than one extremity and often involve the perineum and trunk. The most common forms are Klippel-Trenaunay Syndrome (KTS) and Parkes-Weber Syndrome (PWS).
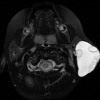
KTS is a combined Capillary-Lymphaticovenous Malformation (CLVM), characterized by capillary staining, venous anomalies of the deep and superficial systems, lymphatic malformations and limb overgrowth involving soft tissue and bone. KTS usually involves the lower extremity and trunk in combination but can also involve an upper extremity. The lymphatic component of the syndrome is prone to infection and internal bleeding while the venous component can be complicated by blood clot formation which can migrate to the lungs.
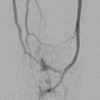
PWS is a combined Capillary-Arteriovenous Malformation (CAVM), characterized by capillary staining, multiple AVMs and overgrowth of the affected extremity. The AVM component of this syndrome is most troublesome with pain, skin breakdown, bleeding and often high output cardiac failure due to the number and size of the arteriovenous shunts.
Treatment of combined malformations includes interventional radiological techniques discussed previously. A multi-disciplinary approach with input form Surgeons, Dermatologists, Hematologists, Radiologists and other specialties, is vital in managing patients with combined vascular malformations.
Sclerotherapy/Embolization Procedures
Treatment is preceded by an outpatient consultation at which time the patient is fully evaluated, the procedure is explained in full and any additional blood tests or radiological examinations are requested.
Radiologically guided treatment for all types of vascular malformation involves percutaneous (through the skin) and endovascular (through blood vessels) placement of needles and catheters to deliver the sclerosant or embolic material to the affected lymphatic or vascular channel. Chemical agents used include Sodium Tetradecyl Sulfate (STS), Alcohol, n-Butyl Cyanoacrylate (n-BCA), Onyx ® liquid embolic agent, Doxycycline and Bleomycin. Other agents used include endovascular coils and endovenous laser.
Delivery of sclerosant can be painful and procedures can be lengthy. For both these reasons, it is preferable to perform sclerotherapy under general anesthesia. Treatment is usually followed by admission for observation with patients normally discharged the day following the procedure.
To arrange a consultation or if further information is required, please contact CVIR (Cardiovascular Interventional Radiology) at: 215-955-6440