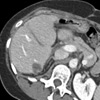
MRI demonstrates a 3 cm posterior renal mass extending from a solitary kidney. The contralateral kidney was resected.

Interventional Radiology


Thermal Ablation
Cryoablation/Radiofrequency Ablation of Tumors: Ablative therapies destroy tumors by achieving extreme temperatures after the tumor is punctured with one or more needles under computed tomographic (CT), ultrasound (US), or magnetic resonance (MR) guidance. Tumors are either heated by application of microwave or radiofrequency energy or frozen during cryoablation. Ablation was initially developed for unresectable hepatocellular carcinoma (HCC). Over time, treatment of small tumors has led to 3 year survival of 67%. Given the success with this tumor, ablation has been used in other organ systems with impressive efficacy. A recent report has demonstrated 100% disease-free and metastasis-free survival using ablation to treat renal masses less than 4 cm in diameter with a median follow-up of 5 years. Patients suffering from excruciating pain from skeletal metastases can be treated with a single session of ablation. Rapid onset of relief typically occurs with significant improvement in both pain and interference of daily activities using standardized scales along with a reduction in opioid requirements. Ablation of lung tumors is another expanding area of clinical practice. Two and five year survival rates following ablation of non-small cell lung cancer of 57% and 27% have been reported.
Case Study


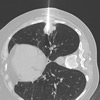
The patient is prone in the CT prior to cryoablation.

At the end of cryoablation, the resulting ice ball encompasses the tumor as well as a 1 cm surrounding margin.

Follow-up CT demonstrates no residual viable tumor.
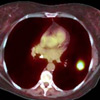
PET/CT demonstrates a hypermetabolic focus in a patient who previously underwent radiation therapy. She was not a candidate for surgery or further radiation.
An expandable ablation electrode is deployed around the tumor.
28 months after treatment, no active disease is present.
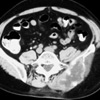
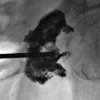
CT scan of a 50 year old male with metastatic renal cell carcinoma. He used a walker during admission to the hospital.
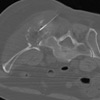
Image during ablation demonstrates an electrode deployed within the tumor. The next morning, the patient walked without assistance or pain.
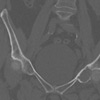
This patient with uterine sarcoma has a destructive metastasis involving the acetabulum. At the time of treatment, she was bedridden, in part to prevent the involved bone from fracturing.
Following cement injection, the patient’s pain was significantly improved and the support provided by the procedure allowed her to walk.
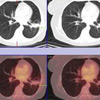
CT reveals a solitary sarcoma metastasis in a patient who has co-morbidities preventing surgery.

Image during ablation demonstrates the electrode deployed within the tumor.

Follow-up CT 3 months later demonstrates necrosis of the tumor with a wide margin