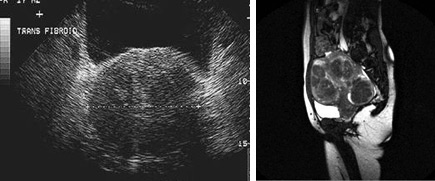
Uterine fibroids (leiomyomas or myomas) are the most common benign (non-cancerous) tumor of the female reproductive tract. Up to 40% of women age 35 and older and up to 50% of African American women have uterine fibroids.
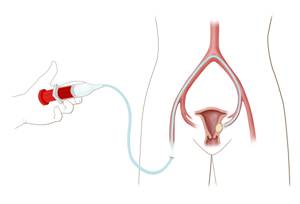
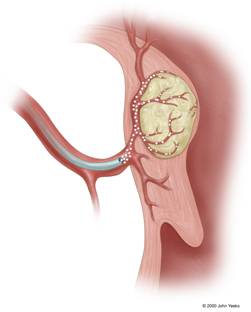
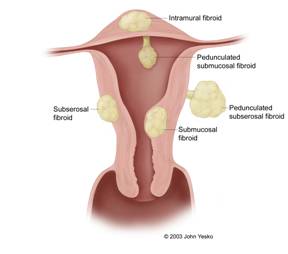
Fibroids may be located within the wall of the uterus (intramural), on the surface of the uterus (subserosal), or beneath the lining of the uterine cavity (submucosal) (Figure 1 to the right). Some fibroids are located on a stalk and are referred to as pedunculated fibroids.
What are some of the symptoms associated with uterine fibroids?
Symptoms associated with uterine fibroids include prolonged, heavy menstrual cycles or menorrhagia, dysmenorrhagia (abnormal bleeding between menstrual cycles), fatigue from iron-deficiency anemia (low blood count), pelvic/back pain, constipation, obstipation (painful bowel movements), dyspareunia (painful sexual intercourse), bloating, and urinary frequency.