
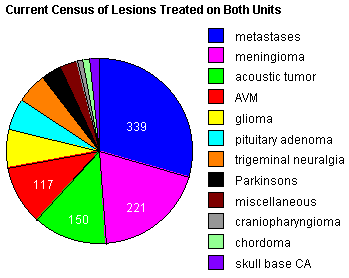
Since of the inception of our program, the radiosurgery team has treated a variety of lesions in over 1150 patients on these units as featured in the pie chart to the right.
The practice of radiosurgery involves the collaborative clinical participation of a neurosurgeon, a radiation oncologist, and a medical physicist. In our division we are fortunate to have on our radiosurgery team the National Chairman of the RTOG (Radiation Therapy Oncology Group), Dr. Walter J. Curran, Jr., who is Professor and Chairman of the Department of Radiation Oncology at Thomas Jefferson University Hospital. Dr. Curran and his staff have a singular commitment to the Radiosurgery program, and in the spirit of this collaborative multidisciplinary team, the Division has participated in national brain tumor trials sponsored by the RTOG.
As our policy, any and all patients referred for consideration of radiosurgery treatment are evaluated by a neurosurgeon and a radiation oncologist. The physician to whom the patient is originally referred then presents the patient’s case at a multidisciplinary brain tumor/ stereotactic radiosurgery board comprised of neurosurgeons, radiation oncologists, neuro-oncologists, neuroradiologists, as well as residents and fellows who participate in case presentation.
This formal review process ensures the most objective and informed treatment decision for each patient. If focused radiation is recommended, discussion is then directed to which technique, either single fraction stereotactic radiosurgery on the LINAC or Gamma Knife, or fractionated stereotactic radiotherapy on the LINAC, is best suited for the treatment of a particular lesion. Each of these dedicated units have unique characteristics which provide benefit when considering treatment. As examples, the Gamma Knife, due its array of very small collimating helmuts, is ideally suited for small lesions or lesions most effectively treated with the highest degree of “fit” or volume of radiation which conforms to the lesion—the “conformality” of the treatment.
If a patients has numerous lesions located in widely separated areas of the brain, the LINAC provides the greatest versatility in targeting all lesions with one frame application for single fraction treatment. If a patient has a tumor near the optic nerves, conventional fraction stereotactic radiotherpy on the LINAC provides the greatest treatment benefit.